


PEST Case 3: The hunt for foreign objects
“A 12-month-old is rushed into the emergency department unresponsive in his mothers arms. He was last seen playing with some toys in the living room. When Mum returned he was unresponsive, lying on the floor.”
Clinical findings
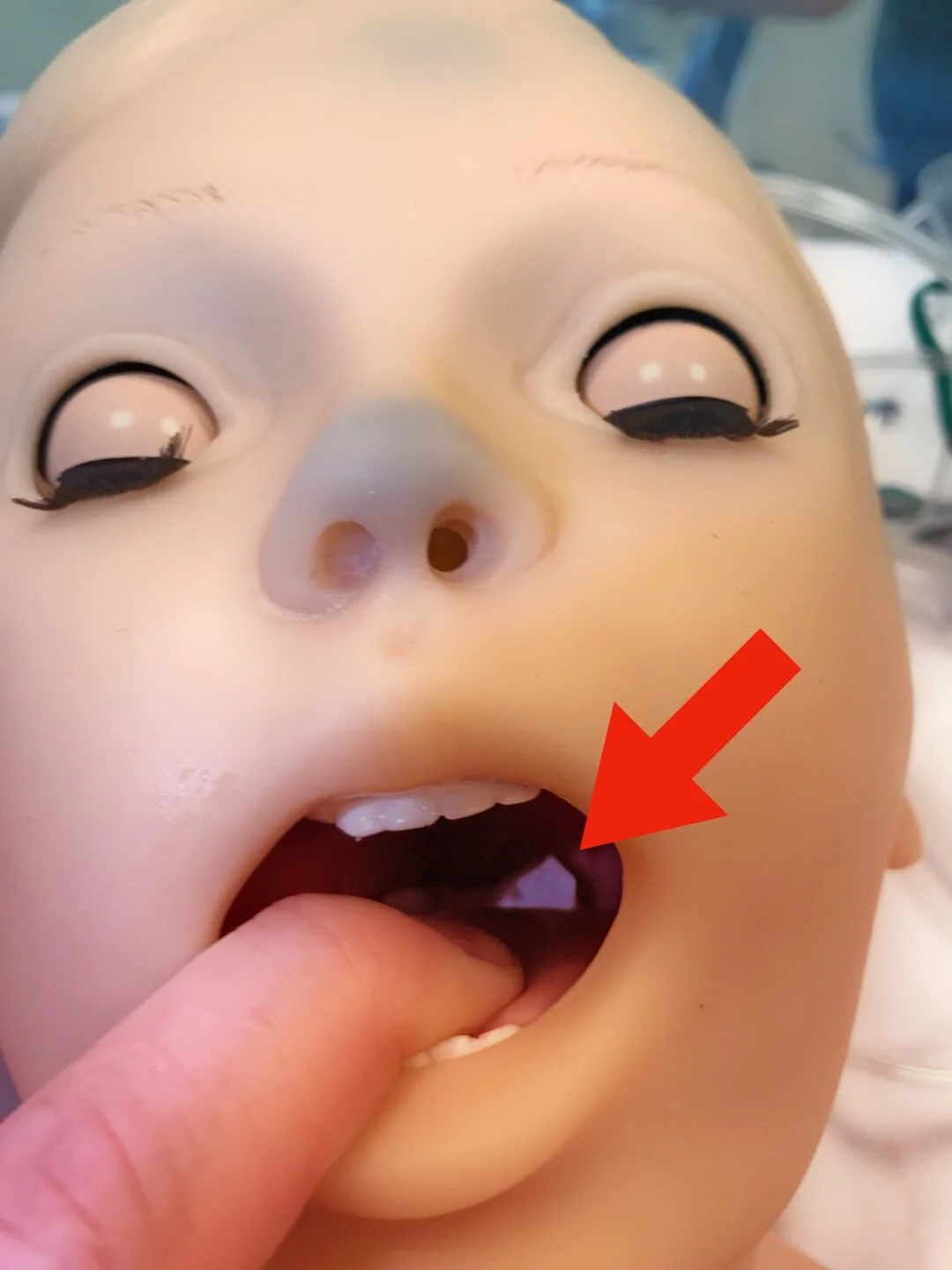
A: Not fogging the mask, no response. Foreign body can be found in oropharynx on close inspection
B: No spontaneous breathing, no air entry on auscultation
C: Cardiac arrest – no output
D: GCS 3/15 – E1 (no response) V1 (no response) M1 (no response); Pupils: 4mm and reactive B/L
E: Temp 36.9°C (mottled & pale)
Observations
SpO2 (not recordable)
RR (not recordable)
HR (not recordable)
BP (not recordable)
CRT 4-5 sec
Diagnosis
Asphyxia secondary to foreign body (FB) inhalation
Why we simulated
Asphyxiation secondary to FB inhalation is a common cause of respiratory arrest in children. FB ingestion is often unwitnessed and may present without an obvious history so clinicians should be mindful of checking the airway and dealing with reversible causes of cardiac arrest. It is important to reassess A, B, C, D and E when running through the cardiac arrest algorithm, particularly after introducing an intervention and especially if there is no improvement. If you think you could be missing something, ask your teammates for their ideas.
Our airway doctor identified the FB, communicated clearly with other team members and removed the obstructing body with forceps. After 3 rounds of CRP, we achieved a return of spontaneous circulation (ROSC) and continued supportive care.
Learning points
1) Foreign body aspiration
Inspect the airway
Do not insert fingers or suction device beyond what you can visualise as you may further displace a FB or cause iatrogenic trauma. If inserting your fingers, do not pass the proximal metacarpophalangeal (MCP) joints beyond the incisors.
Do not jeopardise the airway by unpleasant or frightening interventions, contact a senior anaesthetist/ENT surgeon urgently
Remember, FB inhalation can not be excluded by either a normal physical exam or CXR
Laryngo-bronchoscopy is needed for all children with a history suggestive of FB aspiration
In our case, a FB was visible in the context of an extreme life threat, immediate direct laryngoscopy was performed with a Magills forceps which removed the object successfully
2) ROSC... now what?
Once ROSC is achieved, clinicians must be active in delivering supportive care to ensure the patient remains stable. If the patient is not managed effectively during this time they may easily slip back into cardiac arrest. Re-assess from the top.
A: Do we have a definitive airway? Are effective breaths being delivered? Is there a CO2 detector attached?
B: Equal and effective bilateral breath sounds?
C: Confirm there is a pulse? Check rate, rhythm, QRS complexes on a 12-lead ECG. Measure BP? Check CRT? Consider IV maintenance fluids?
D: Pupils equal and reactive to light? AVPU?
E: Measure temperature? Check BM?



Staff feedback
“Sometimes the sickest patient can arrive 'out of the blue' requiring urgent team intervention to consider what is happening. Algorithm for cardiac arrest. The need to be very wary once ROSC has occurred as there is potential for deterioration.”
“Always proactively manage a return of spontaneous circulation (or you might lose it again!)”
“It helped increase my confidence in team working during an arrest.”













