#PEST2015: Major Trauma
““A 14-year-old pedestrian hit by a van in hit & run incident ~40mph. Loss of consciousness at scene. Scooped & ran as felt too unstable for transfer to Major Trauma Centre (MTC).””
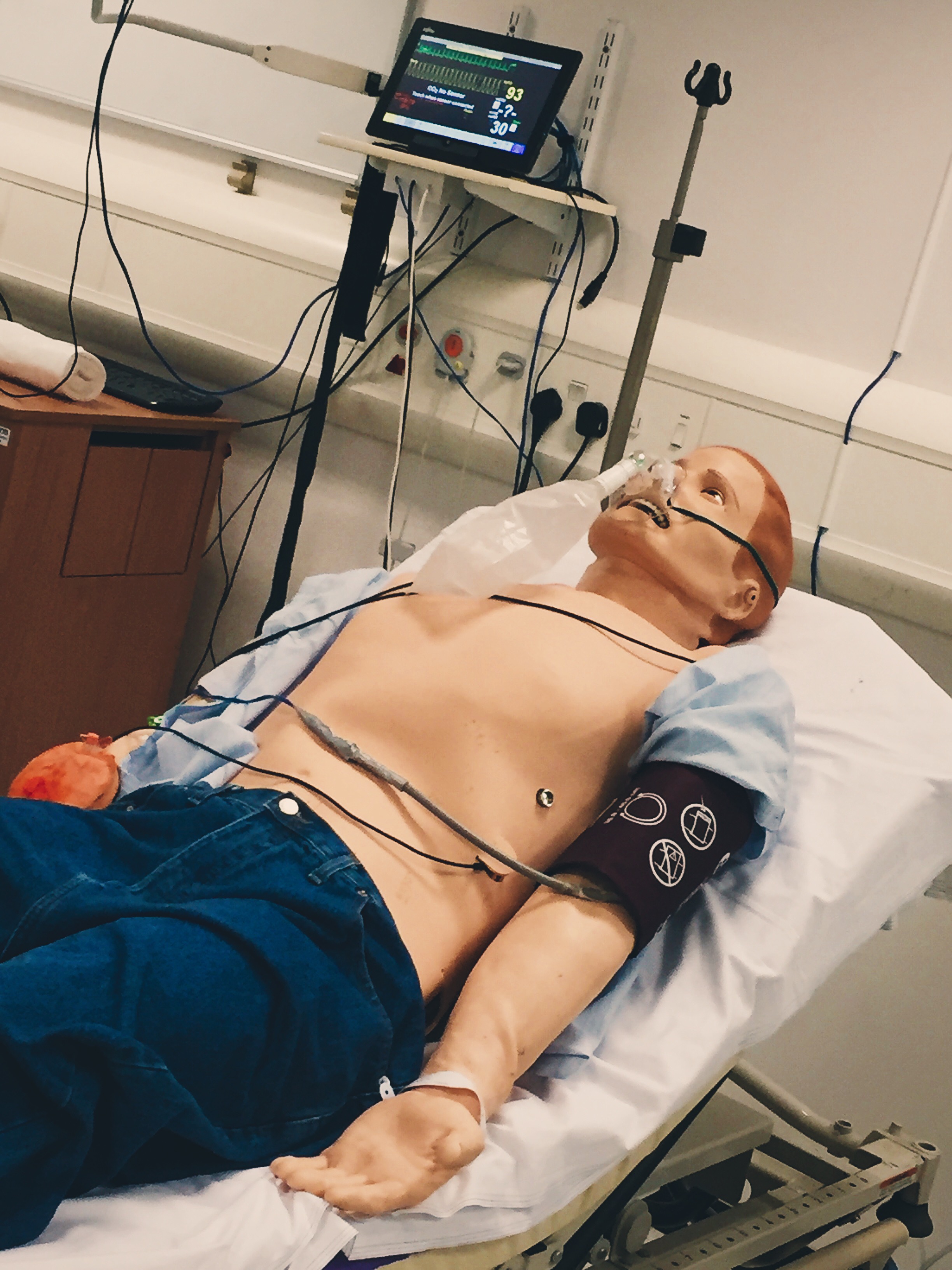
Observations
RR 30, SpO2 91% in air
HR 110, BP 100/40, CRT 3 secs
A[V]PU, GCS 10 (E3 M5 V2), PERL 3mm bilat
Clinical findings
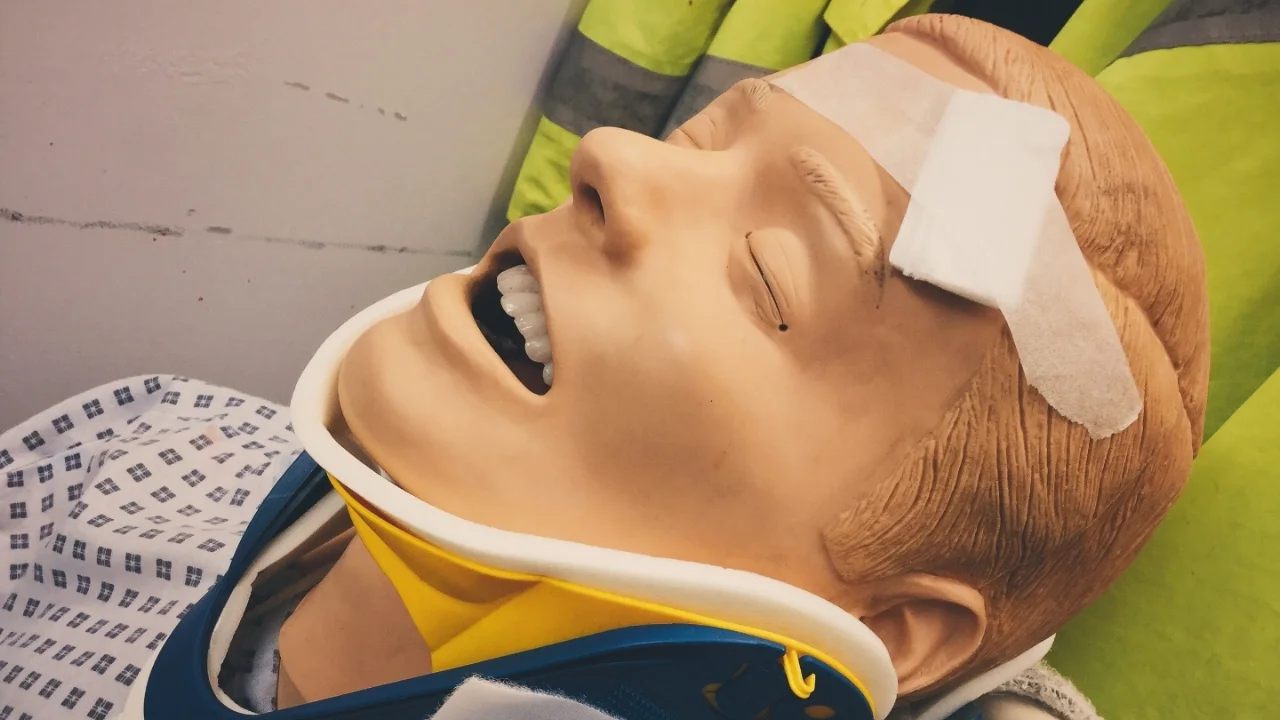
Moaning, incorrectly applied c-spine immobilisation.
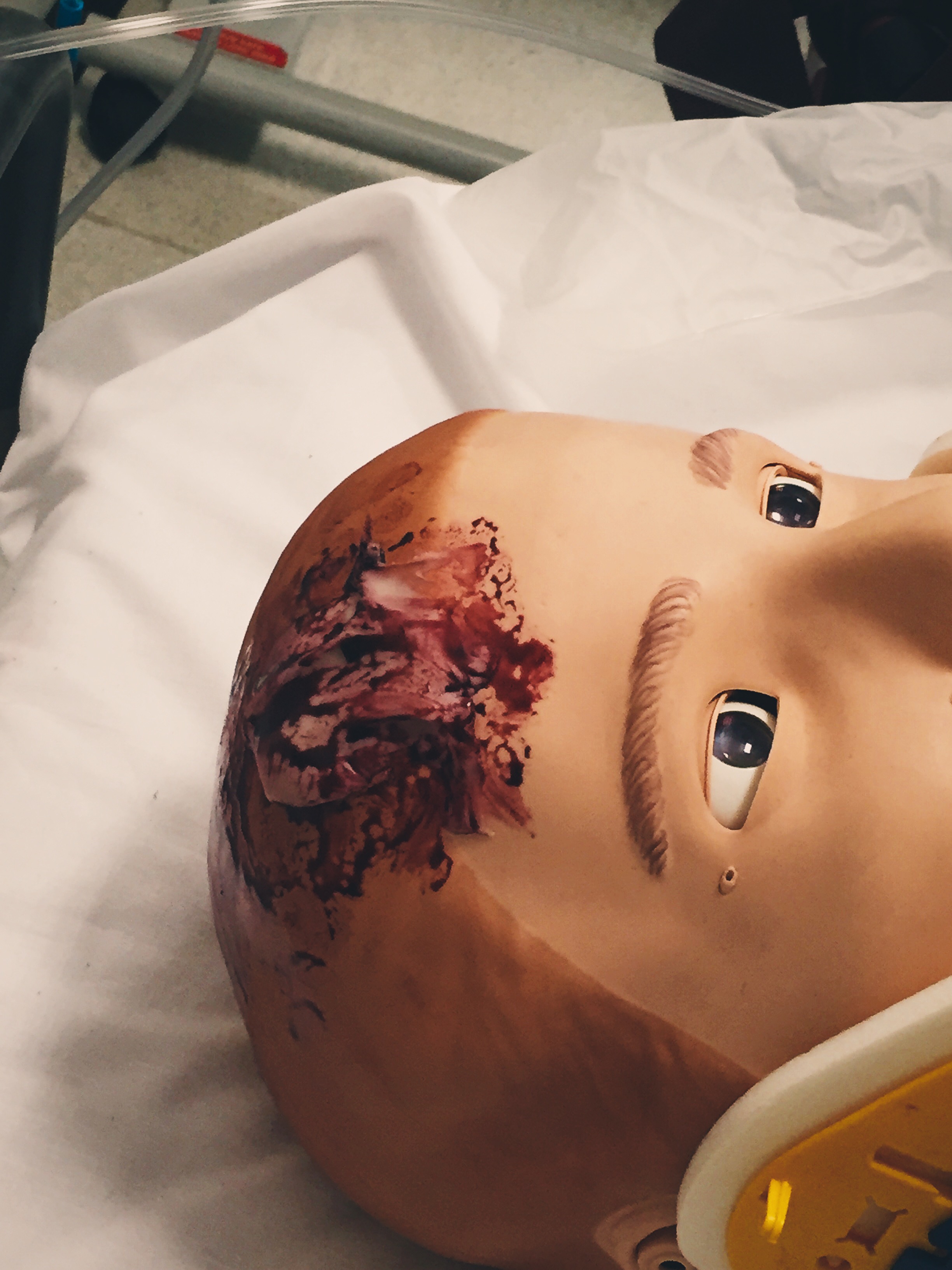
Bruising & wound to scalp, bruising over abdomen & pelvis, open fracture right lower leg.
Why We Simulated?
"A significant proportion of severely injured children were not conveyed to hospital by ambulance”
Almost 30% of paediatric major trauma does not present to a MTC (TARN, 2012). Children with very significant injuries can present at any hospital so it is essential that all units are able to provide initial trauma care.

Learning Points
Familiarise yourself with equipment before you need to use it on a patient
When your hospital cannot provide definitive management for a time critical injury consider carefully how much investigation & management should be initiated before transferring to that definitive care
Positive Feedback
Recognition of patient with multi-system injuries that needed transfer to trauma centre.
Managed task focussed specialty doctor well, did not get distracted from treatment priorities.
Identified time critical head injury and started neuroprotective measures.