


#SimBlog: Paediatric monthly round-up
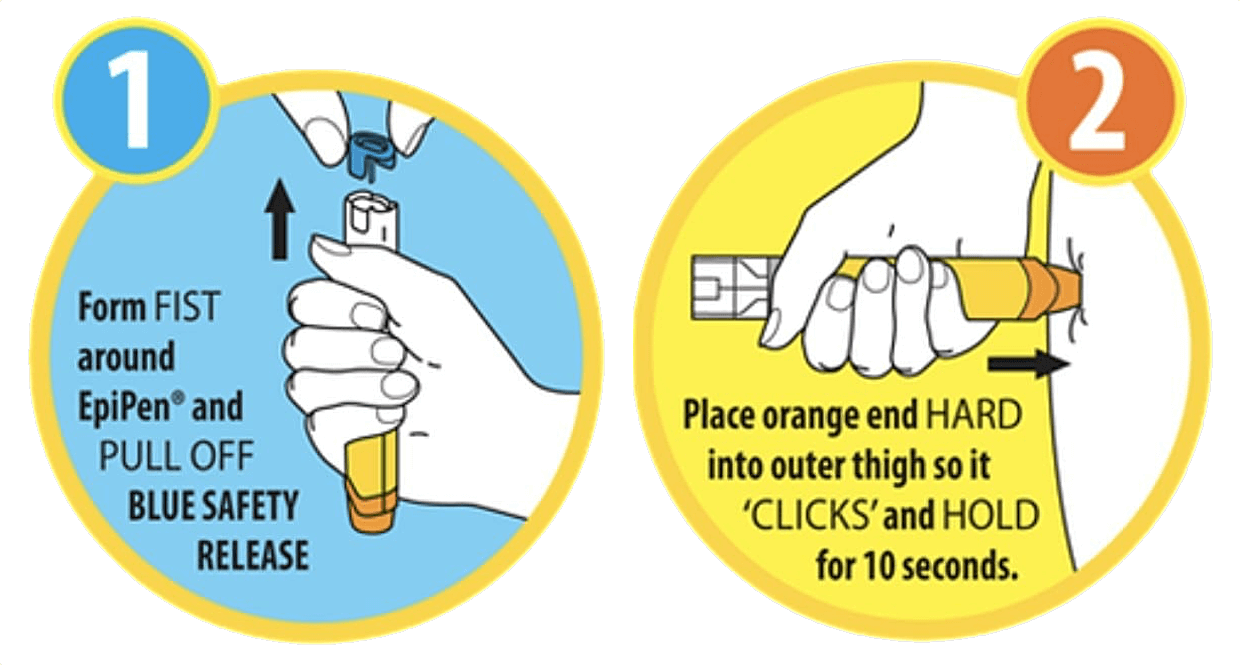
EpiPen? EPICpen!
Scenario: 5-year-old boy admitted with an infected big right toe. Known penicillin allergy but prescribed IV augmentin. Location: High Dependancy Unit (HDU) in the Paediatric ED. Date: 10th Sept. 2018
Intended learning outcomes…
Initial structured A-E of a collapsed patient
Know where the difficulty in breathing and anaphylaxis grab box is in the Paediatric ED
Administration of IM adrenaline
Learner-led outcomes…
Always check drug allergies and medication when prescribing
You can give multiple doses of adrenaline if required
Know how to prep and deploy the adrenaline auto-injector: don't lose the patient and your thumb!
There’s no ‘i‘ in ‘Team’
Scenario: In-situ simulation of a 2-year-old boy who had been admitted with throat infection and febrile convulsion. Had a further episode of febrile convulsion on the Childrens Short Stay Unit (CSSU) during a period of observation. Location: CSSU then Paediatrics ED. Date: 24th Sept. 2018
Intended learning outcomes…
Interdepartmental communication between CSSU and Paeds ED, e.g. tannoy/emergency call bell
Human factors including communication, leadership, role allocation and prioritisation of jobs across CSSU and Paeds ED staff
Acute management of a febrile seizure including location and use of seizure grab box and crash trolley
Appropriate escalation of care
Learner-led outcomes…
Need for 'crowd control': many people present after crash buzzer to manage one febrile seizure (re: team behaviours)
Conversation about when and how it would be appropriate to move to the ER (re: clinical care systems)
Grab box: know where it is and what it contains (re: latent environmental factors & individual clinical competence)
Cardiac monitors: need to make sure cardiac leads are present on CSSU as they were not (re: latent environmental factors)
Relationship between CSSU and ED at both the staffing and equipment level, e.g. Lorazepam located in ED (re: team behaviours & clinical care systems)
Communication between staff: there was a lot of "can someone just..." communication. Recognition of need to be specific with task request and need for feedback loops in communication (re: team behaviours)
Where did the Team Leader go?
Scenario: 3-year-old child with a background of atopy, egg allergy and under the Respiratory and Allergy teams. Admitted overnight and has had six salbutamol nebulisers, two atrovent nebulisers, and prednisolone – which he vomited up. Concern as he is becoming more tired. Location: HDU in Paediatric ED. Date: 1st Oct. 2018
Intended learning outcomes…
Importance of handing over potentially sick children
Assessment and management of a tiring atopic child with difficulty in breathing
Location and contents of difficulty in breathing grab box
Recognition of local and national guidelines
Learner-led outcomes…
Need to delegate tasks more specifically, e.g. “Emily, can you get the cannula trolley?” (re: team behaviours)
Graded assertiveness: importance to verbalise your thought process and not be afraid to speak up (re: team behaviours)
Where did the Team Leader go? Recognition of need to communicate task allocation clearly and know where key members of the team are (re: team behaviours)
The WETFLAG computer algorithm is difficult to access and not working adequately (re: latent environmental factors)
Location of DIB box and IV salbutamol (re: clinical care systems)
When the team receive an important piece of information (blood gas) this should be communicated to everyone effectively (re: team behaviours)
Exposing the truth…
Scenario: 4-year-old child with a 2-day history of raised temperature, decreased eating/drinking and becoming more lethargic. Location: HDU in Paediatric ED. Date: 15th Oct. 2018
Intended learning outcomes…
Importance of completing A-E assessment
Not to become fixated on oxygen saturations
Location and contents of sepsis grab box
Application of The Sepsis Six
Learner-led outcomes…
Knowing names is important in acute situations
Expose the child-there may be a hidden rash!
Low oxygen sats could be due to a number of reasons: equipment failure, reduced perfusion, actual low oxygen saturations
Not to fixate on something such as low oxygen saturations: treat it and move on
Vocalise your concerns, e.g. “Adam, I am concerned that the blood gas shows a metabolic acidosis with raised lactate”




