
Based at the University Hospitals of Leicester, we serve the educational needs of healthcare practitioners in Acute & Emergency Medicine across the East Midlands, UK

Lecture 6: Acute Confusion & Dementia
“Your grandma is taken to your neighbouring Emergency Department (ED) by ambulance because she’s just not feeling right…”
Once there’s, she’s as pleasant and sweet as she was when you visited her last Sunday (which you now do regularly because you’ve noticed that she’s not as sharp as she used to be.)
However she’s also a 'vague historian' and gives several different reasons why she called the ambulance. No one bothers to check on her ability to remember or to execute basic tasks. And no one bothers to contact you to get some collateral history. She stays around for a long time and has a lot of investigations – but no food or water.
Eventually she’s discharged home to follow up with her primary care provider – even though no one asked if she has one or sent any information to him. And things don’t turn out so well. In fact, she, your grandmother, becomes the subject of that phrase, “remember that patient you sent home the other day… ?"
Delirium is a Medical Emergency!
EPIDEMIOLOGY
Prevalence: 1-2% of older people in community; 14-56% of hospital inpatients.
Incidence: from 6-56% in general hospital admissions; 15-53% in postoperative setting; 70-87% in intensive care.
Typically, predisposing non-modifiable factors (dementia, serious illness) interact with precipitating, modifiable factors (sedatives, infections, surgery, electrolyte abnormalities).
RISK FACTORS
When people first present to hospital or long-term care, assess them for the following risk factors. If any of these risk factors is present, the person is at risk of delirium:
Age 65 years or older.
Cognitive impairment (past or present) and/or dementia. If cognitive impairment is suspected, confirm it using a standardised and validated cognitive impairment measure.
Current hip fracture.
Severe illness (a clinical condition that is deteriorating or is at risk of deterioration).
Observe people at every opportunity for any changes in the risk factors for delirium.
PRESENTATION
Cognitive function: for example, worsened concentration, slow responses, confusion.
Perception: for example, visual or auditory hallucinations.
Physical function: for example, reduced mobility, reduced movement, restlessness, agitation, changes in appetite, sleep disturbance.
Social behaviour: for example, lack of cooperation with reasonable requests, withdrawal, or alterations in communication, mood and/or attitude.
SOME FACTS
Neuroimaging has identified structural changes, including cortical atrophy, ventricular dilatation and white matter lesions, to be predictors of delirium.
Current evidence suggests that disruption of neurotransmission, inflammation or acute stress responses might contribute markedly to the development of delirium.
Delirium is not always transient and reversible, and it can result in long-term cognitive changes.
DELIRIUM FACTORS
Patients who are highly vulnerable may be older, have severe dementia, and have multiple comorbidities. In these patients (see Diagram 1), a relatively benign insult, such as a small dose of narcotic medication, can precipitate delirium.
Patients who are less vulnerable to developing delirium, like those who are younger and have little comorbidity burden, require higher doses of noxious stimuli (e.g. severe sepsis) to develop delirium.
Because older patients are more likely to have multiple vulnerability factors, they are disproportionately more susceptible to becoming delirious compared to younger patients. For this reason, nursing home patients are especially vulnerable.

Diagram 1. The interrelationship between patient vulnerability and precipitating factors in the development of delirium. Patients who have little vulnerability require significant noxious stimuli to develop delirium (black arrow). Conversely, patients who are highly vulnerable require only minor noxious stimuli to develop delirium (grey arrow).
PREDISPOSING FACTORS
Demographic
Advanced age
Male gender
Comorbidity
Dementia
Number of comorbid conditions
Severity of comorbid conditions
Chronic kidney disease
End-stage liver disease
Terminal illness
Medications and Drugs
Polypharmacy
Baseline psychoactive medication use
History of alcohol or other substance abuse
Functional Status
Functional impairment
Immobility
Sensory Impairment
Hearing impairment
Visual impairment
Decreased Oral Intake
Dehydration
Malnutrition
Psychiatric
Depression
PRECIPITATING FACTORS
Systemic
Infection
Inadequate pain control
Trauma
Dehydration
Hypo- or hyperthermia
Metabolic
Thiamine deficiency (Wernicke encephalopathy)
Hepatic or renal failure
Electrolyte disturbances
Hypo- or hyperglycaemia
Thyroid dysfunction
Medications and Drugs
Medications and medication changes
Recreational drug use or withdrawal
Central Nervous System
Cerebrovascular accident
Intraparenchymal haemorrhage
Subdural/epidural hematoma
Seizures and postictal state
Meningitis/encephalitis
Cardiopulmonary
Acute myocardial infarction
Congestive heart failure
Respiratory failure
Shock
Iatrogenic
Procedures or surgeries
Indwelling urinary catheters
Physical restraints
Dementia-related Delirium
Dementia is a chronic, progressive syndrome characterised by cognitive dysfunction. It affects each person in a different way, depending upon the impact of the disease and the person’s personality before becoming ill (adult attachment profiles: secure, dismissing, fearful and preoccupied).
Dementia is also the commonest predisposing cause for developing delirium, with a higher rate of hospitalisation, institutionalisation and death.
PRESENTATION
Hyperactive: restless, agitated, hyper vigilance, hallucinations and delusions.
Hypoactive (commonest): lethargic, quiet, slow response, little movement.
Mixed
PATHOPHYSIOLOGY
Cholinergic system: anticholinergic and anti-parkinsonian drugs can cause delirium.
Inflammation: proinflammatory cytokines in trauma, infection, surgery.
Acute stress: raised cortisol (impaired feedback).
Neuronal injury: hypoxia, hypoglycaemia, other metabolic derangements.
Neuroimaging: associated cortical atrophy; hypoperfusion in functional imaging.
PREVENTION
Avoid benzodiazepines or anticholinergics.
Hospital Elder Life Programme: maintaining orientation to surroundings; meeting needs for nutrition, fluids and sleep; promoting mobility within the limitations of physical condition; and providing visual and hearing adaptations for patients with sensory impairments (OR 0.6, CI 0.39-0.92).
Manage pain, constipation, retention of urine.
Avoid lines/tubes/restricting mobility – if possible.
ENVIRONMENTAL CONSIDERATIONS
Supporting people who are living with dementia is one of the biggest challenges that our health and social care system will face in the 21st-century. There is rightly much emphasis placed upon how we deliver care, but the environment within which we deliver care, can also make an enormous difference to the quality of people's lives.
There is clear evidence to show that if you get the environment right (see Table 1), this has benefits not only for people who use care services, but also for their families, friends and staff. This document from the Department of Health provides extensive research into the development and design of a dementia-friendly department.
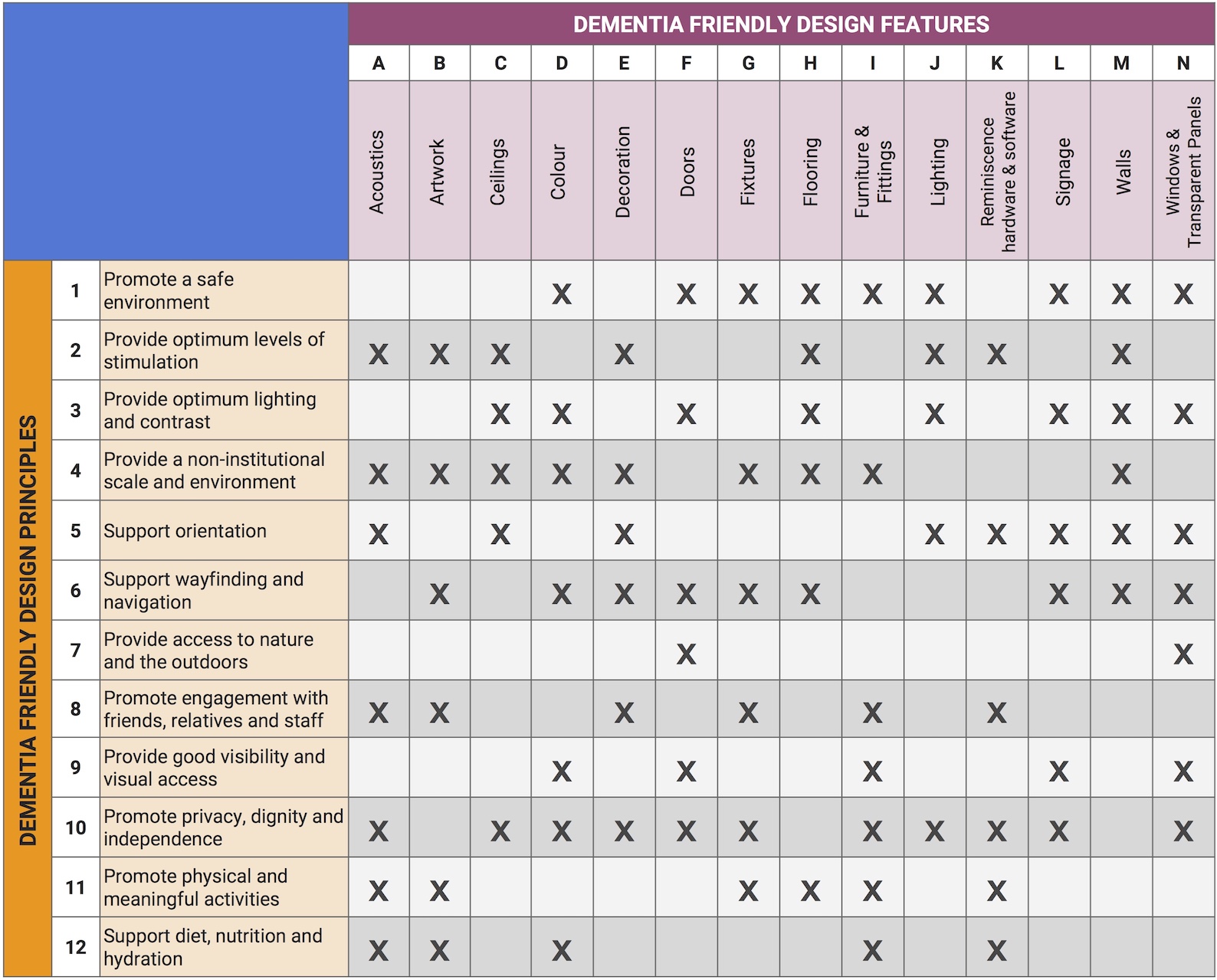
Table 1. Core dementia-friendly design features
DIAGNOSTIC CRITERIA
A: Disturbed consciousness
B: Change in cognition
C: Rapid onset (hrs to days); tends to fluctuate daily
D: Evidence from Hx, PE, investigations
direct effect of medical condition
substance intoxication or medication use
developed after substance withdrawal
more than one aetiology (medical condition + medication side effect)
Diagnostic and Statistical Manual of Mental Disorders, 4th edn, text revision (DSM-IV-TR®; American Psychiatric Publishing, Inc., Arlington, VA).
#1: Alertness
This includes patients who may be markedly drowsy (e.g. difficult to rouse and/or obviously sleepy during assessment) or agitated/hyperactive.
Observe the patient. If asleep, attempt to wake with speech or gentle touch on shoulder. Ask the patient to state their name and address to assist rating.
Normal (fully alert, but not agitated, throughout assessment) = 0
Mild sleepiness for <10 seconds after waking, then normal = 0
Clearly abnormal = 4
#2: AMT4
Age, date of birth, place (name of the hospital or building), current year.
No mistakes = 0
One mistake = 1
Two or more mistakes/untestable = 2
#3: Attention
Ask the patient: "Please tell me the months of the year in reverse order, starting at December." To assist initial understanding one prompt of "what is the month before December?" is permitted.
Achieves 7 months or more correctly = 0
Achieves less than 7 months, or refuses to start = 1
Untestable (cannot start because unwell, drowsy, inattentive) = 2
#4: Acute Change or Fluctuating Course
Evidence of significant change or fluctuation in: alertness, cognition, other mental function (e.g. paranoia, hallucinations) arising over the last 2 weeks and still evident in last 24 hours.
No = 0
Yes = 4
4 or above: possible delirium +/- cognitive impairment.
1-3: possible cognitive impairment
0: delirium or cognitive impairment unlikely (but delirium still possible if #4 information incomplete)
DELIRIUM MIMICS
The diagnosis of delirium is made on the basis of clinical history, behavioural observation and cognitive assessment. The history should confirm that an acute change in baseline cognitive function has occurred.
It is important to ascertain the time course of the mental status changes, as well as any history of intercurrent illnesses, medication usage (including any changes in medication and use of over-the-counter and herbal products), alcohol withdrawal, and changes in the environment. Conditions that mimic delirium (see Table 2) should be excluded.
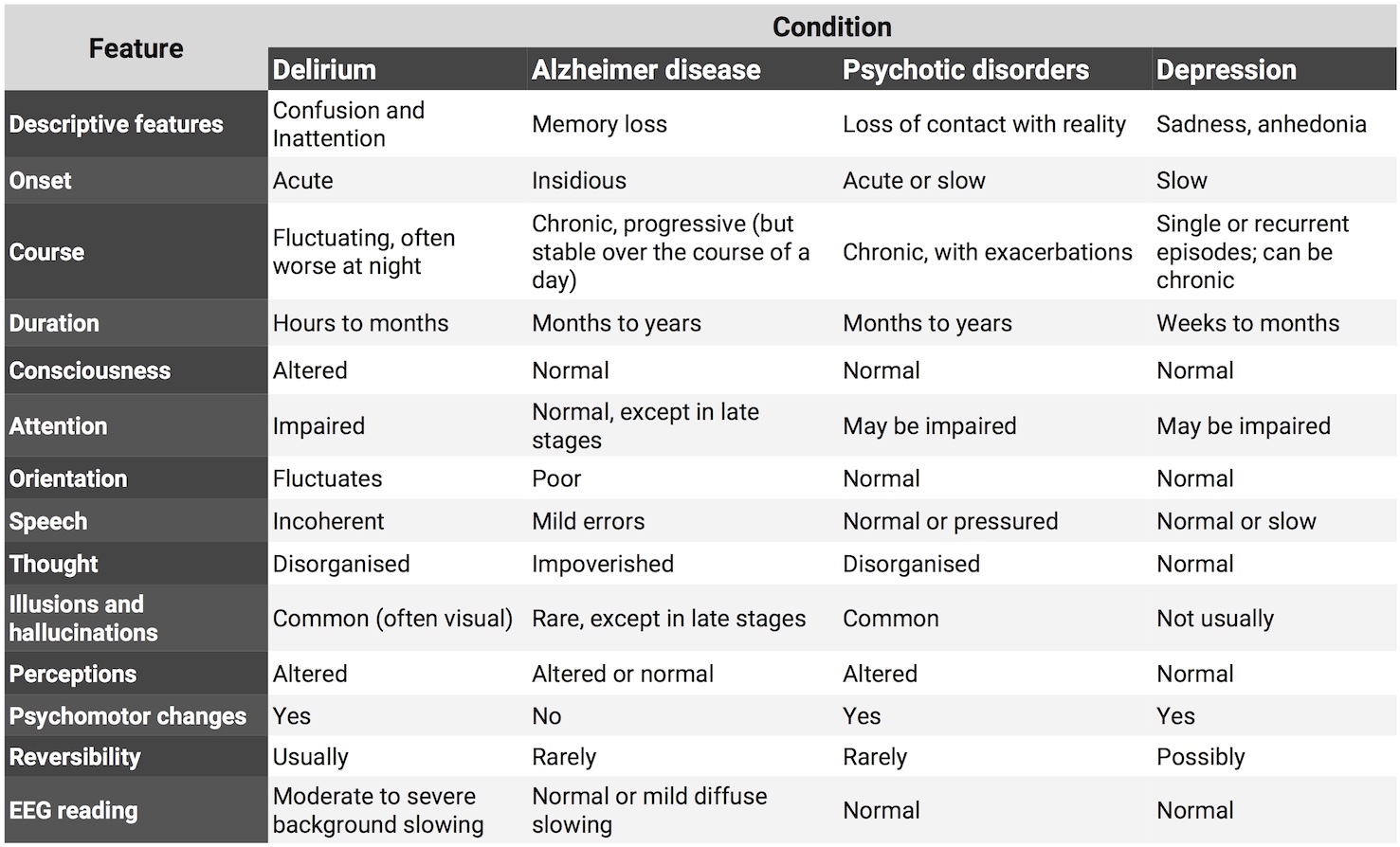
Table 2. Differentiating features of conditions that mimic delirium
The 2-step approach to delirium surveillance for the emergency department: the Delirium Triage Screen (DTS) and the Brief Confusion Assessment Method (bCAM). See the original journal for more details.
Diagram 2. Delirium Triage Screen (DTS)
Step 1 (DTS) can be integrated into the nurses’ triage assessment. If the DTS result is negative, then delirium is ruled out and no additional testing is needed. If the DTS result is positive, then a confirmatory delirium assessment such as the bCAM should be performed.
Both assessments use the Richmond Agitation Sedation Scale (RASS), which assesses for arousal and ranges from −5 (coma) to +4 (combative); a score of 0 indicates normal level of consciousness (see the originating journal for more details).
Diagram 3. Brief Confusion Assessment Method (bCAM)
INVESTIGATIONS
CT – 7% pickup
FBC, U&E, gases
CXR, urine as indicated clinically
APPROACH
Try non-pharmacological first: reorientation, behavioural intervention; clear instructions & good eye contact.
Address sensory impairment – visual and auditory.
Avoid physical restraints that cause tethering.
Search for underlying cause.
MANAGING DELIRIUM
Identify and treat underlying condition + O2, Glucose, nutrition, hydration, electrolyte balance, manage constipation.
Mortality rates following admission 10-26%.
Manage acute agitation: haloperidol or olanzapine; risk of dystonia, strokes, prolonged QT; lorazepam not first line (over sedation).
OUTCOMES
Aspiration, pressure ulcers, pulmonary embolism, poor intake; more severe the episode, worse the outcomes.
Persistent functional and cognitive loss (persistent delirium).
New diagnosis of dementia after hospitalisation.
Delirium is an important determinant of hospital stay, mortality, rates of nursing home placement, functional & cognitive decline – marker of hospital quality.
DELIRIUM INDICATORS: STRUCTURE & PROCESS
'Structure' in this usage relates to human resources (staff availability and training), the physical environment of care, and funding: the context in which care is provided.
'Process' relates to how the system works: the policies and procedures by which care is provided.
Presence of established policies for the management of people with CI, for their support persons/families, for assessment of behavioural disturbances, for in-ED delirium prevention, and for pain assessment.
THE DAY YOUR GRANDMOTHER SHOWS UP…
So… you decide to make some changes in your department.
You educate your medical and nursing colleagues about the prevalence of CI in older patients – and how frequently we miss its many manifestations.
You develop policies to routinely screen for cognitive impairment and functional decline and to access collateral informants and to prevent further decline in the Emergency Department.
You support the development of an interdisciplinary team (RNs, OTs, SWs) with which you can share the load of caring for these fascinatingly complex patients…
Grandmother shows up… and it's a different story 😉
VIDEOS
Acute Confusion & Dementia
Dr Jay Banerjee & Prof. Simon Conroy discuss the signs and symptoms of older patients with acute confusion, and how to assess for dementia.
Confusion: delirium, dementia or both?
Dr Jay Banerjee, Consultant in Emergency Medicine at Leicester Royal Infirmary gives a summary of his talk at #GEMcon16 about managing the confused patient in ED.
[LIVESTREAM] Confusion: delirium, dementia or both?
Taken from the Periscope livestream of Dr Jay Banerjee's talk at #GEMcon16 on managing the confused patient in the ED. (NB: only a partial talk due to technical issues with the video stream)
Delirium Awareness
Animated video from the Dementia Together NI team to raise awareness of Delirium, its signs, and symptoms. To encourage family/carers and Health and Social Care staff to raise any concerns they may have about possible delirium.
What is Delirium?
Delirium is a sudden disturbance in mental abilities that can last for hours to days. Some patients experience hyperactive symptoms and some patients experience hypoactive symptoms, whereas some experience both.
Myths and MSUs
This MiniGEM explains how and when to diagnose UTI in older patients, and common pitfalls to avoid!
Post-operative Delirium
#ShareTheOrange
What It's Like To Be In A Coma?
REFERENCES
Fong, Tulebaev, Inouye. Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev Neurol. 2009 April; 5(4): 210-220. doi: 10.1038/nrneurol. 2009.24
Han et al. Diagnosing delirium in older emergency department patients: validity and reliability of the delirium triage screen and the brief confusion assessment method. Ann Emerg Med. 2013. November; 62(5): 457-465. d.o.i: 10.1016/ j.annemergmed.2013.05.003
Han et al (2010). Delirium in the Older ED Patient. Emerg Med Clin North Am. 2010 Aug; 28(3): 611–631
Schnitker L, Martin-Khan M, Burkett E, Brand C, Beattie E, Jones R, et al. Structural Quality Indicators to Support Quality of Care for Older People with Cognitive Impairment in Emergency Departments. Academic Emergency Medicine 2015;in press
Schnitker L, Martin-Khan M, Burkett E, Beattie E, Jones R, Gray L. Process Quality Indicators Targeting Cognitive Impairment to Support Quality of Care for Older People with Cognitive Impairment in Emergency Departments. Academic Emergency Medicine 2015;in press
FURTHER READING
#LightningLearning: Delirium [#EM3]
#FrailtyFriday: Dementia [#EM3]
American Delirium Society [more videos]
Communicating about Dementia [Alzheimer's Society]
Delirium: Prevention, Diagnosis and Management [NICE Guidance]
Dementia-friendly Health and Social Care Buildings Environments [DoH]
PODCASTS
#FrailtyFriday: Delirium [#EM3]
Acute Confusion in the Emergency Department [#EM3/RCEM]
Communicating about Dementia [Alzheimer's Society]
QUIZZES
Try out the following online quizzes provided by The University of Nottingham: