#SimBlog: Festive Fever
WARNING: this post pre-dates SEPSIS 3.0 & may refer to older definitions
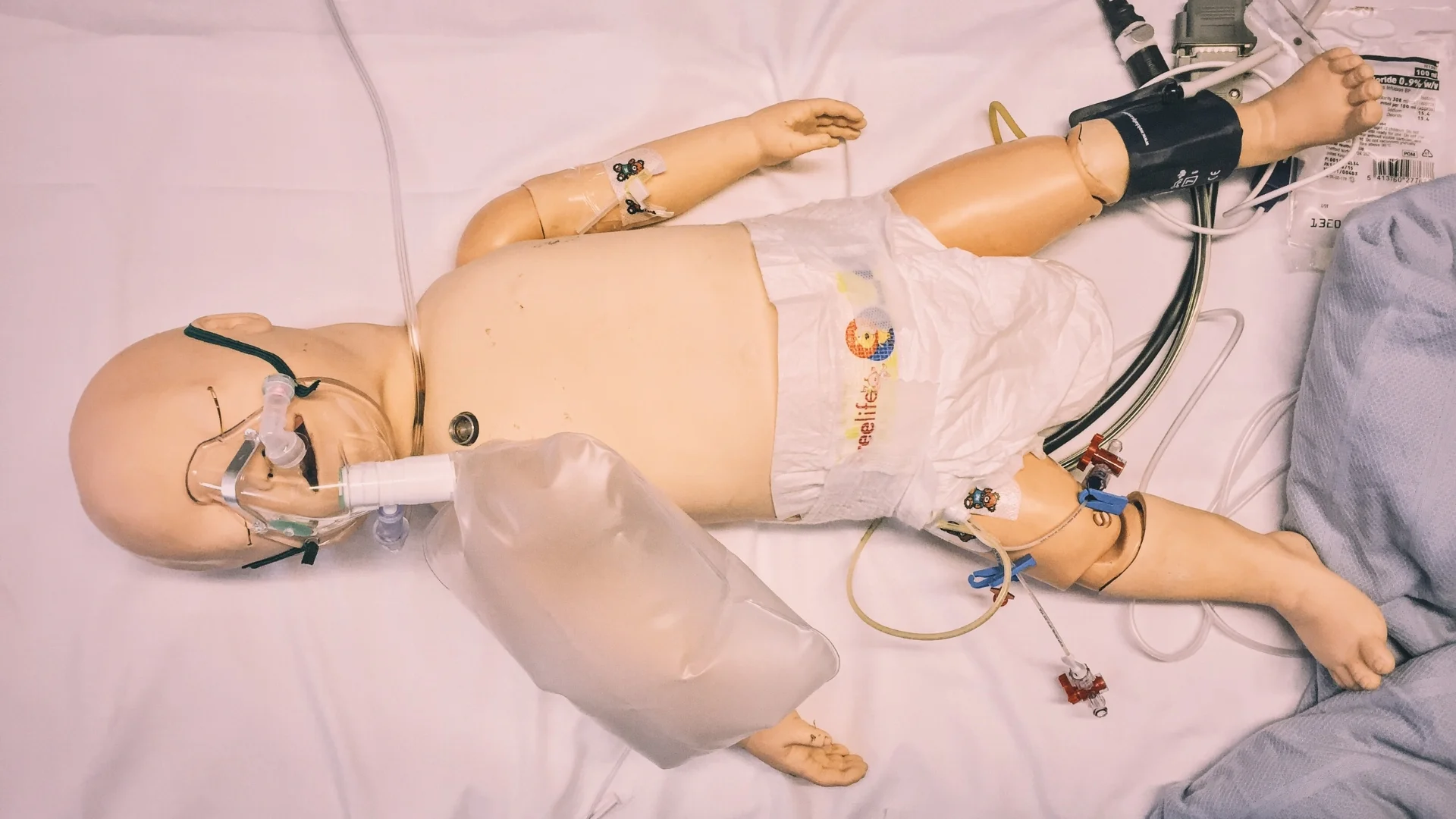
““78-year-old male admitted from his residential home with a 1-day history of being generally unwell and confused.””
Observations
A – Patent, self maintaining
B – RR 25, SpO2 94% in air
C – HR 121, BP 91/65
D – E3, M5, V4
E – Temp 38.9°C, BM 8
Why We Simulated?
The way we stratify sepsis is changing. Once you have identified a patient as being SIRS positive and that infection is likely you now need to look for the sepsis Red Flags. The presence of any Red Flag symptoms triggers the IMMEDIATE commencement of the Sepsis 6.



Sepsis Red Flags
Immediate:
SBP <90 mmHg or >40 mmHg fall from baseline
MAP <65 mmHg
Heart rate >131 per minute*
New need for supplemental oxygen to maintain saturations >90%
Respiratory rate >25 per minute*
AVPU = V, P or U*
POCT (commonly available):
PaO2/FiO2 ratio <300 (mmHg) or <39.9 (kPa)
Lactate >2.0 mmol/L
Radiology (only if clinically indicated, e.g. SpO2 <90%):
Bilateral pulmonary infiltrates AND new need for supplemental oxygen to maintain oxygen saturations >90%
““Every year in the UK there are 150,000 cases of sepsis resulting in 44,000 deaths.””
Laboratory (unless POCT available):
Creatinine >176.8 μmol/L
INR >1.5
aPTT >60s
Platelet count <100 x 109/L
Bilirubin >34.2 μmol/L
Urine output monitoring:
Urine output <0.5 mL/kg for two consecutive hours.
References:
- Sepsis Trust UK – http://sepsistrust.org
Learning Outcomes
We have a new Sepsis Screening and Action Tool – so make yourself familiar with it!
Know your team – introduce yourself to everyone and make sure you know their names.
In any patient you diagnose with sepsis, ask yourself “could this be a life-threatening sepsis mimic?”
Positive Feedback
Recognition of sepsis & Sepsis 6 delivered within 20 minutes of patient arrival.
Good communication with patient by all team members.
Doctor verbalised significantly abnormal blood results.