#SimBlog: Head Injury & NOACs
““73-year-old male with who had a head injury 2 weeks ago now presents with 1-day history of confusion and difficulty walking.””
Observations
A – Patent, self-maintaining
B – RR 14, SpO2 98% in air
C – HR 80, BP 170/95
D – GCS 12/15 (E3, M5, V4)
E – Temp 36.9°C
Clinical findings
Confused speech
Disorientated
Evidence of healing wound left aspect of forehead
Why we simulated?
We are seeing an increasing number of patients within the Emergency Department (ED) who are taking novel oral anticoagulant drugs (NOACs).
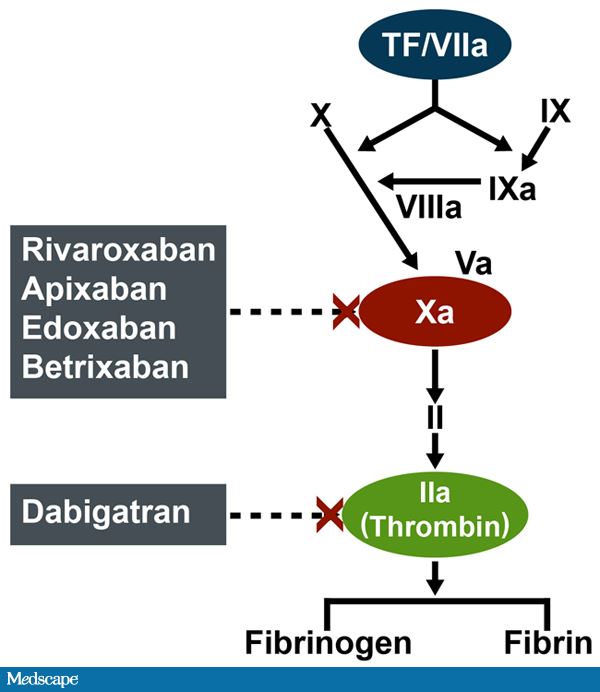
There are two types of NOAC based on their mechanism of action. Dabigatran is a direct thrombin inhibitor, RivaroXaban and ApiXaban are factor Xa inhibitors. These drugs provide a relatively predictable anticoagulant effect and thereby reduce the need for regular monitoring associated with warfarin.
There is currently debate ongoing with regards to the risk of haemorrhage for patients with head injury. Ultimately your department will have its own policy, but I suspect for many this will include a CT Head.
Another cause for concern has been a lack of specific antidotes to reverse the anticoagulant effect. There are several under development and these are likely to be available in your department soon.

Table from London Medicines Evaluation Network Summary
Further Reading:
- London Medicines Evaluation Network Review: Summary of NOAC Antidotes
- Lightning Learning: NOACs
Learning outcomes
It is useful to assign a named team leader to ensure someone is keeping an overview of the patient's care.
When assessing risk of bleeding in patients on NOACs time since last dose is important.
In UHL there is a Prothrombin Complex Concentrate (PCC) pack that needs to be printed off and filled in before PCC is requested from Haematology.
Positive feedback
Excellent communication with patient throughout the scenario.
Early involvement of haematology.
Good preparation by staff pre patient's arrival.