#SimBlog: Ruptured Ectopic Pregnancy #1
““21-yr-old female, self-presented to ED with a 6-hour history of abdo pain and vomiting. She’s also had 2 loose stools.””
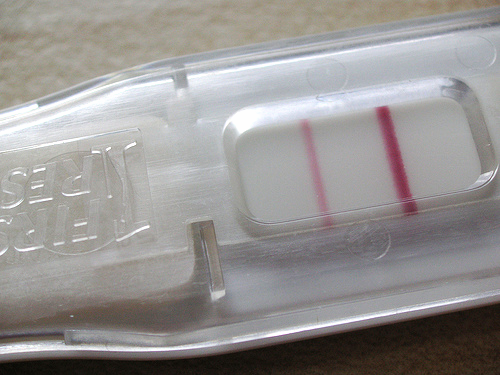
Assessment Bay observations revealed an EWS of 5. She has been moved to the Emergency Room, ?Sepsis. No history of PV bleed. LMP 2 weeks ago. Not on OCP but denies sexual contact.
Observations
A – Clear and self maintained
B – Rate 26, SpO2 98%.
C – Pulse 110, BP 89/60.
D – GCS 15 pupils equal reactive
E – Temp 36.9°C
Clinical Findings
Tender Abdomen
Localised guarding to LIF
Bowel sounds present
Why We Simulated?
"Emergencies in Pregnancy are very challenging. Patients’ symptoms can be misleading or confused with normal pregnancy, their vital signs are normally altered, the physical exam can often be more difficult, their lab values are harder to interpret and imaging algorithms for pregnant patients are very complicated.” – (Emergency Medicine Cases)
Not to mention that the patient may not know they are pregnant or may not wish to disclose they could be.
Positive Feedback
Recognised the acuity of the patient.
Considered possibility of pregnancy early on.
Asked for senior review when needed.
Learning Points
It is reasonable to think ahead to a most likely diagnosis or worst case scenario, however by keeping to an "ABCD" structure you are less likely to miss things.
Keeping to a structure can also allow you to assess a patient even if you are feeling out of your depth.
Imaging may have a role in the investigation of abdo pain, however in this case AXR and CXR should only be considered if they will affect management.