
Based at the University Hospitals of Leicester, we serve the educational needs of healthcare practitioners in Acute & Emergency Medicine across the East Midlands, UK

Limb Pain, Swelling, Traumatic Limb & Joint Injury
“DVT affects approximately 1 in 1000 people in the UK each year. This leads to the deaths of 25,000 people each year due to pulmonary embolism.”
CAP 20 – Limb Pain and Swelling Atraumatic
CAP 33 – Traumatic Limb and Joint Injuries
EM Curriculum: (click to view)
Background
Limb pain can be caused by a number of differing conditions. These vary from pain caused by direct trauma to the musculoskeletal system to the first sign of multi-system auto-immune medical disease. Swelling, skin changes and difficulty in moving the affected limb are often accompanying symptoms.
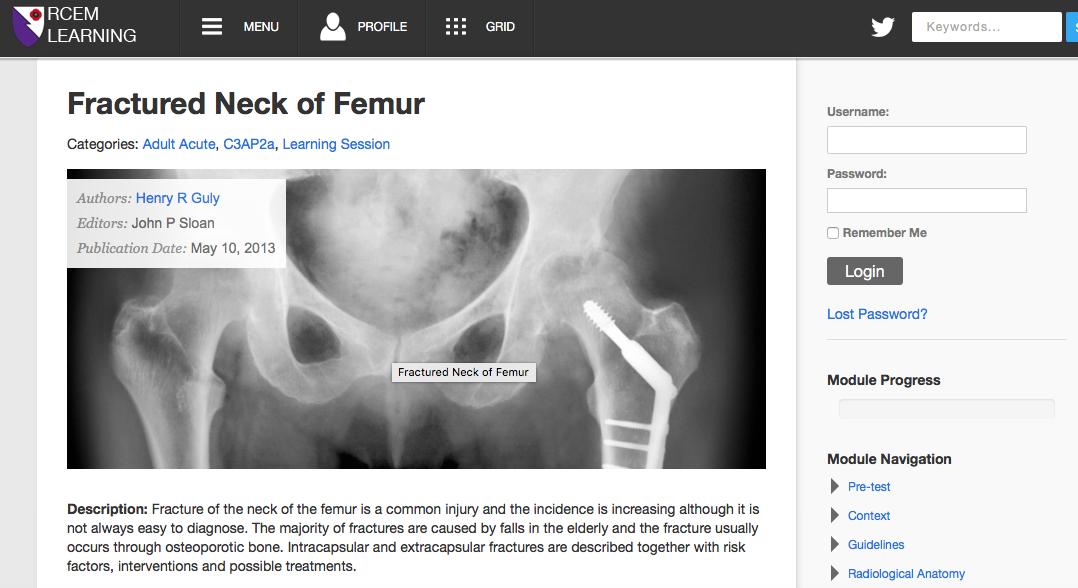
A fractured neck of femur is a particularly important injury. 70-75,000 people in the UK will suffer from a fractured neck of femur each year, and mortality from this fracture can be as high as 35% (NICE).
Fractured neck of femur accounts for 87% of all fragility fractures, with osteoporosis being one of the major risk factors. The cost of these fractures to the NHS is approximately £384 million.
Assessing patients with limb injuries necessitates thorough anatomical knowledge. It is important to know which structures can be damaged, as missing a nerve or tendon injury can have significant consequences on function.
Learning Outcomes from completing the tasks
Know how to assess, investigate and manage swelling and pain in the lower limb to include DVT.
Identify a patient with a fractured neck of femur and describe its management.
Describe how acute ischaemic limb presents and how it is managed in ED.
Identify different skin infections that commonly present to ED and their management including necrotising fasciitis.
Learning Outcome from face-to-face teaching
Revise the medical conditions presenting with severe limb pain.
Describe the pathophysiology and the aetiologies of limb oedema.
Identify different injuries to the limbs to include soft tissue injuries and bone injuries.
Describe the management of various injuries to the limb.
Illustrate how to perform a fascia illiaca block.
Tasks
Complete the following before the face to face session:
Task 1: VTE in the ED
Duration: 20 mins
This blog entry from RCEMFoamed covers VTE in the ED, it also covers the Well's Score, D-dimers, PE's and NOACs.

Bonus Task:
Duration: 5 mins
This video from RCEM15 (Manchester) covers the latest developments in the management of VTE.
Task 2: #NOF
Duration: 60 mins
This module covers fractured neck of femurs in some detail, because of the significance of these injuries it is well worth spending the time on it.
Task 3: Limb Ischaemia
Duration: 10 mins
This short entry from Sketchy Medicine covers the features of an acutely ischaemic limb and touches on the management. Once again their cartoons make excellent resources for visual learners.

Task 4: Soft Tissue Infections
Duration: 7 mins
This short podcast gives the take home points from a talk given at the RCEM15 Belfast conference. It covers antibiotics for cellulitis, why worsening swelling might not need admission, necrotising fasciitis.

#EM3 Content
Lightning Learning:
Summary Block
Simblog:
Summary Block










Mini Teaches:
Foundation Course Module:
The Minor Injuries module from our foundation course contains some other resources that are useful for working in minors. If you haven't worked in the ED as a foundation trainee or just want a refresher it is worth taking a look.

CASE DISCUSSION
We have written a series of interactive cases (wikis) with short answer questions to be answered by trainees prior to the face to face teaching sessions. Currently this is only available to East Midlands Trainees.
Answer one or two questions before attending the face-to-face teaching session. Add comments to answers already given if you think it's appropriate. We will also provide tutor comments. If you find good resources that answer a question why not include links in your comment.
Part of the face-to-face teaching will be spent discussing the case(s) below:
“A 24 year old presents to the ED after falling off his skateboard attempting a stunt. His only apparent injury is to his right lower leg.”
“A 82 years old lady presents to the ED after rolling out of bed at her residential home. She has been complaining of left leg pain since it happened a few hours ago but has been able to weight bear and walk with a little support.”
Additional Resources
Here are some extra resources to review if you want more information:
RCEM Learning:
UPPER LIMB NERVE INJURIES:
A quick summary of nerves that can be injured, the mechanisms and examination findings. Curtesy of @drsarahedwards.
BMJ LEARNING (REQUIRES SUBSCRIPTION):
Shoulder Examination (Video)
Hip Examination (Video)
Knee Examination (Video)
Ankle Examination (Video)
ANATOMY FOR EMERGENCY MEDICINE:
Need a refresher on your anatomy? These videos are aimed at teaching anatomy relevant to emergency medicine and to cover the CEM syllabus.They are well worth a watch if you are a bit rusty and make for good revision for MCEM part A if you are considering emergency medicine. Specific videos include:
They are also available via iTunes.
TEACH ME ANATOMY:
Another visual resource for anatomy revision.
SKETCHY MEDICINE:
If you are a visual learner then this website is a must.
JOINT REDUCTION VIDEOS:
These excellent videos by @Lmellick from the US show how to reduce some of the common large joint dislocations that we perform in the ED. If you check out his youtube channel there are many more videos on a range of topics.
COURSE FEEDBACK
Once you have worked through the exercises, discussed the example cases and attended the face-to-face teaching, please complete the following form: