


#MiniTeach: The Trouble With Trampolines
"A 15-year-old girl was bouncing on a trampoline when she fell, injuring her back."
She was immobilised by the ambulance crew with a collar, blocks and a spinal board.
1. What further information would you like to have regarding the mechanism of injury?
What actually happened to cause her to fall?
Did she fall on the trampoline or off the trampoline?
Was there anyone else on the trampoline with her at the same time and if so how big were they? (This is important because bouncing with others can significantly increase the forces involved in each bounce – see attached paper).
How did she land and what did she land on?
What sort of trampoline was it and were there any safety features present? (Gym versus garden, cushioning, safety net, supervision).
2. What should your examination entail?
Use the ATLS approach:
Assess airway with C-spine – maintain in-line immobilisation.
Breathing – Look, Feel, Percuss, Auscultate.
Circulation – Pulse, Cap refill time, Blood Pressure, Colour. Assess abdomen, pelvis, long bones and for any external bleeding.
Disability – GCS, pupils, check for head injury. Perform a comprehensive neuro-exam including power, sensation, tone, reflexes. If the patient is stable, ATLS would recommend performing a log-roll and checking for bruising, deformity, tenderness, sacral sensation
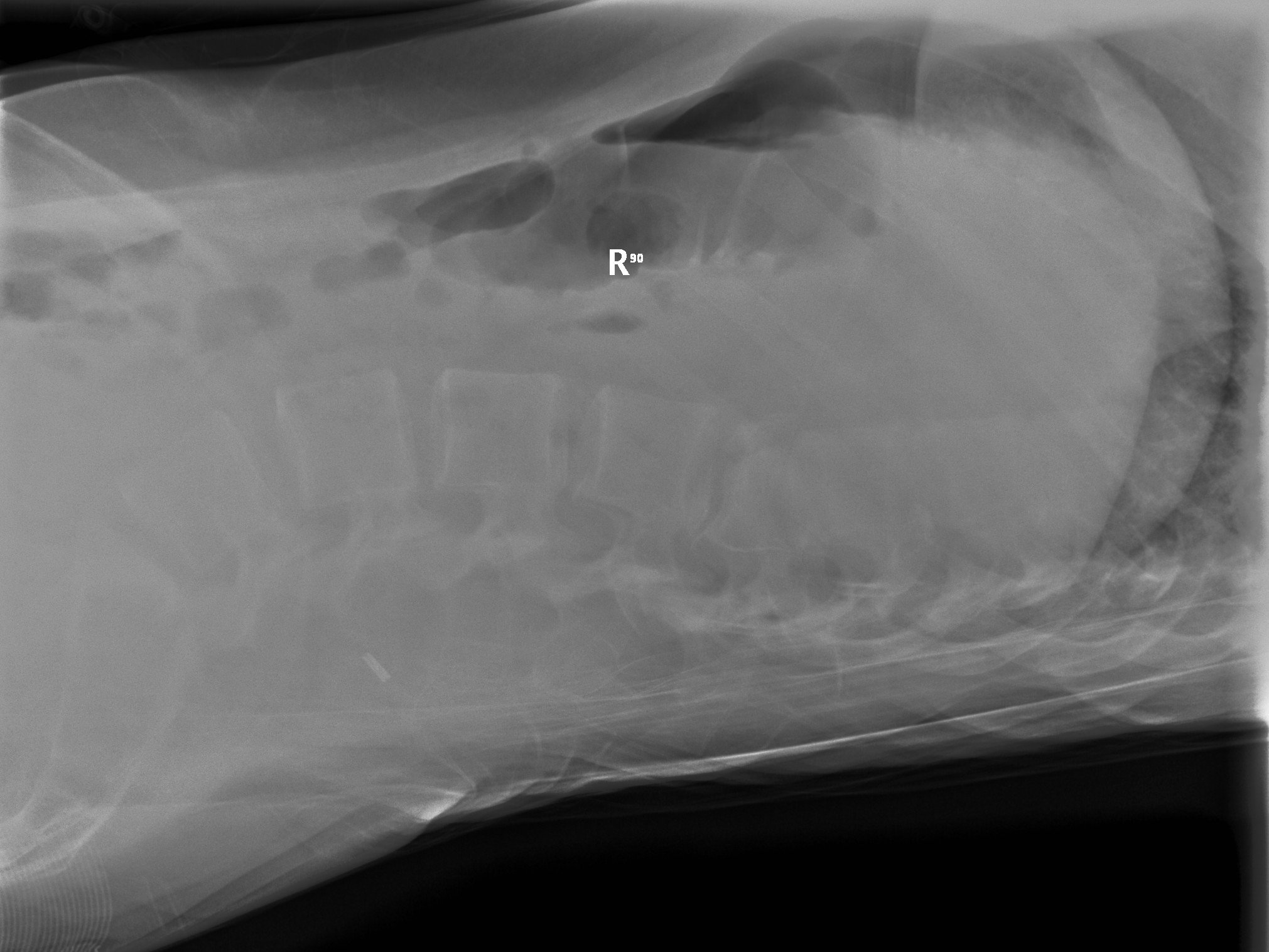
3. What does the X-ray show?
The X-ray shows a compression wedge fracture of L1.
4. How can you classify thoraco-spinal fractures?
This is a bit of a mean question as there have been numerous classification methods in the past, none of which completely fits the bill.
The Denis classification uses the three column system, which divides the vertebral column up into three longitudinal columns, anterior, middle and posterior. The severity of fracture depends on how many columns are disrupted. This system has met with criticism because the middle column is an anatomical arbitrary entity.
The more recent A-O system encompasses a total of 27 different types of fracture based on whether they are a compression (type A), distraction (type B) or rotation (type C) fracture.
For those with exams looming or an orthopaedic fascination, have a look at: Classification of thoracolumbar fractures and dislocations by the National Center for Biotechnical Information (NCBI)
5. What makes a spinal fracture stable or unstable?
The spine is stable if it can resist axial compression forces, axial distraction forces and torsional forces. An injury which renders the spine unable to resist any of these forces is an unstable injury.
6. What would be the further management for this patient?
Maintain immobilisation and examine closely for other injuries. Ensure adequate analgesia.
Ensure that the patient is referred to orthopaedics and liaise with a paediatric radiologist regarding further imaging.
She went on to have a CT scan (see attached image), which showed a comminuted wedge fracture with displacement of fragments into the spinal canal. (Most visible on the MRI).
Following this, she had internal fixation.




